
Peritoneal Dialysis (PD) Modalities
Peritoneal dialysis can be performed manually or via automated systems. Manual PD is termed continuous ambulatory peritoneal dialysis (CAPD). Automated peritoneal dialysis (APD) can be performed as continuous cyclic peritoneal dialysis (CCPD), intermittent peritoneal dialysis (IPD), tidal peritoneal dialysis (TPD), or continuous flow PD (CFPD)1,2. The PD Plus modality uses both manual and automated exchanges.
Continuous ambulatory peritoneal dialysis (CAPD)
CAPD was introduced in 1976 by Popovich and Moncrief3 and later modified by Oreopoulos4 as a wearable and portable form of dialysis, not requiring any equipment other than the disposable solution bags and a line to connect the bag to the patient’s catheter. CAPD was based on the concept of equilibrium dialysis. Briefly stated, when 2 liters of dialysis solution are infused into the peritoneal cavity of an average adult and allowed to dwell for 4 – 6 hours, there is virtual equilibration of the concentration of small solutes between plasma and dialysate (D/P = 1). It was theoretically predicted that an average size anuric patient would maintain a steady-state blood urea nitrogen (BUN) of approximately 28 mmol/L using CAPD and capable of achieving 10 L of equilibrated effluent. This led to widespread use of the standard CAPD regimen consisting of 4-5, 2-L exchanges/day (Figure 1). The procedure involves the infusion of the solution (approximately 10 min), a dwell period (3-6 hours) and drainage of the dialysate (10 – 20 min)5,6.
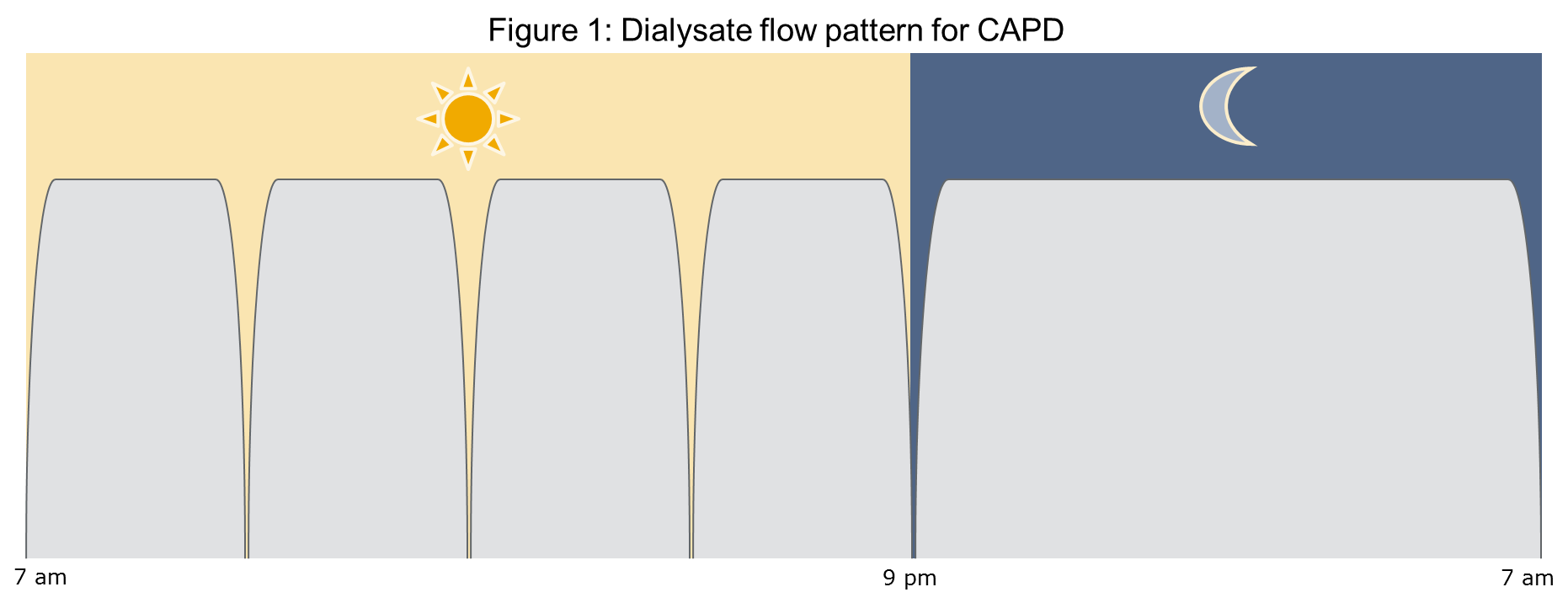
Due to variation in patient size and body composition, they might not be able to achieve enough solute clearance per day with the standard CAPD prescription. They may thus require more, frequent exchanges or larger infusion volumes5.
The simplicity of CAPD, its low cost, and the associated freedom from machines made CAPD a very popular form of chronic PD. In addition, CAPD can maintain a steady physiological state, control fluid volume and blood pressure in most patients7.
Continuous cyclic peritoneal dialysis (CCPD)
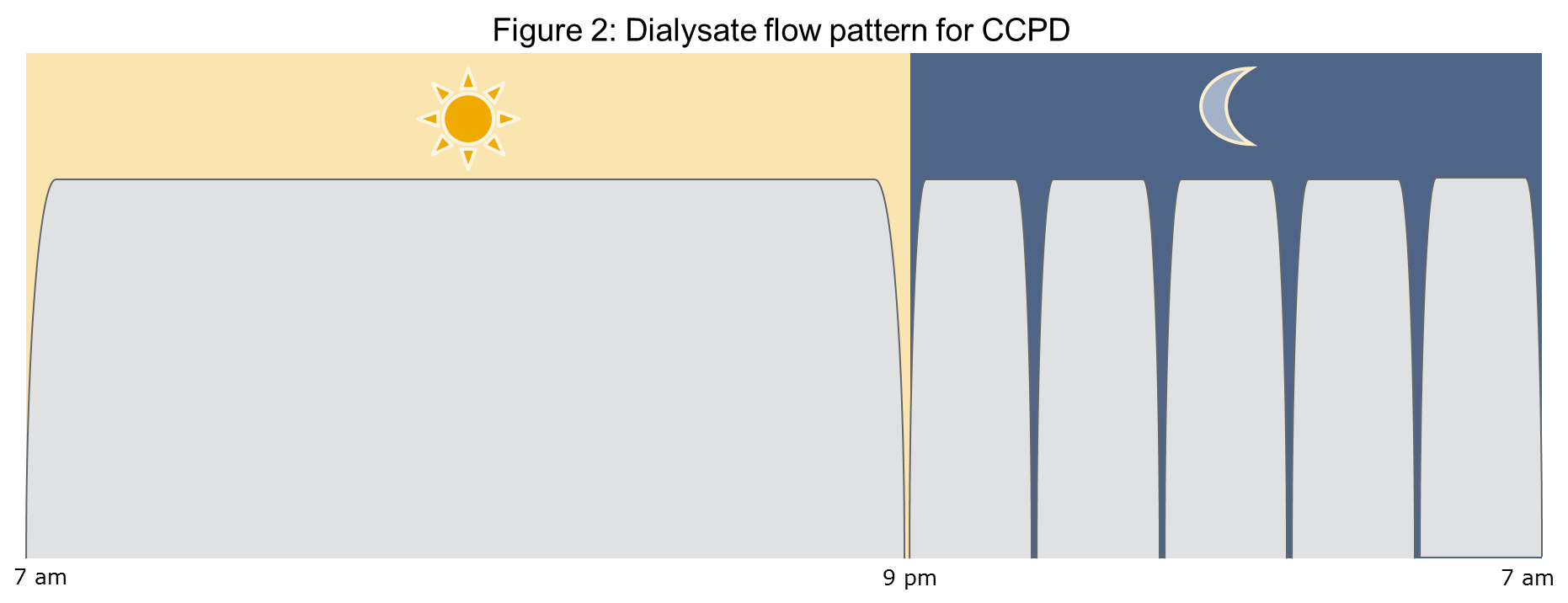
This modality of automated peritoneal dialysis (APD) was introduced in the late 1970s with the aims of achieving higher solute and fluid removal compared to CAPD and to automate the procedure with a simple cycler while the patient sleeps8. The system gained immediate popularity to treat infants and children. CCPD allows greater flexibility in the number and volume of exchanges during the night without taxing the patients’ time. Larger volumes are also better tolerated in the supine position. All connections and preparation of equipment usually takes place at bedtime. Consequently, there is better control of the environment and less patient fatigue. CCPD minimizes direct contact between patient and connections compared to CAPD, reducing the risk of touch contamination9,10–12.The typical prescription consists of three to four exchanges during the night of volumes between 2 and 3 L each. In addition, there is a long day dwell with 1.5 to 2 L of dialysate (figure 2)5.
Intermittent peritoneal dialysis (IPD)
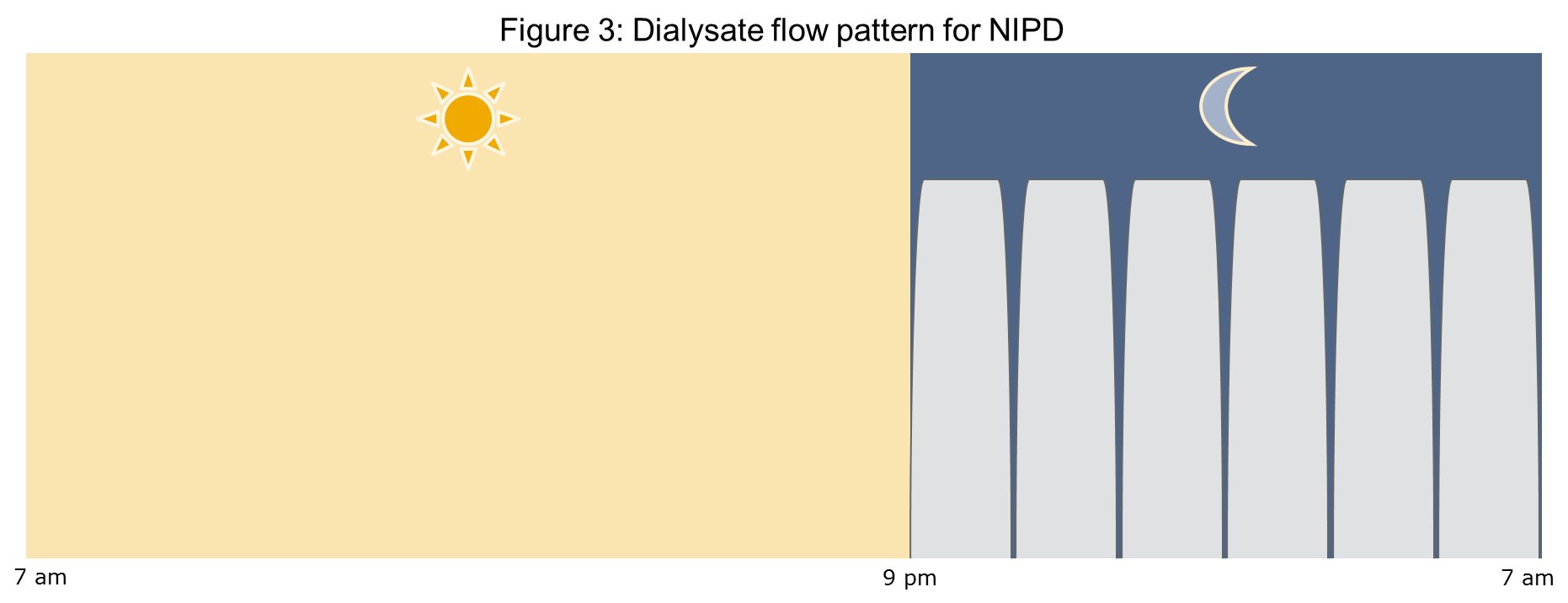
IPD was the first APD modality for chronic use. It remained popular until the 1980s when more effective forms of PD were introduced. IPD generally consists of frequent, short cycles performed over 8 – 10 hours per session, three times weekly5. The peritoneal cavity was drained and “dry” between sessions. If IPD is practiced on a nightly basis only, it is referred to as nocturnal IPD (NIPD). The principal disadvantages of IPD are limited solute removal, especially of larger solutes and high cost due to large volumes of solution. NIPD is mostly reserved for patients with high solute transport and limited ultrafiltration, since the short cycles of NIPD can achieve better ultrafiltration than the longer cycles of CAPD or CCPD. The total volume of dialysis fluid exchanged per treatment ranges between 8 L and 12 L6,13. The regimen for NIPD is shown in figure 314.
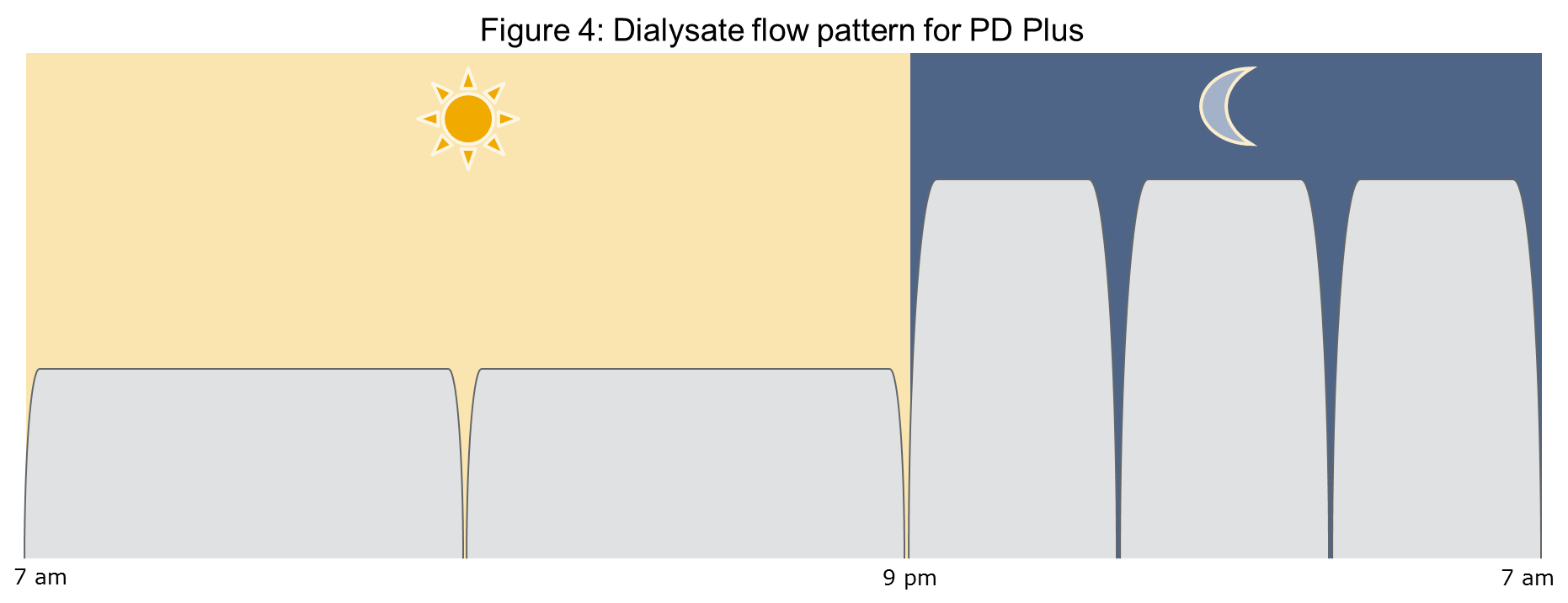
PD Plus (figure 4) comprises CCPD with an additional exchange during the late afternoon or evening5. There are 3 or 4 exchanges at night, with 2 to 3 L per exchange for a total of 8 to 10 hours. The long daytime dwell is divided into two shorter exchanges that may be performed manually or can be cycler assisted. The interruption of the long diurnal dwell of CCPD can improve both clearance and ultrafiltration. PD Plus limits daytime exchanges to less than 7 hours. This exchange is also commonly referred to as a “pause”. Another benefit of this modality is that it makes use of lower volume day exchanges to improve patient comfort and larger exchange volumes in the supine position at night. PD Plus is indicated for larger patients, high transporters, and anuric patients.
Tidal peritoneal dialysis (TPD)
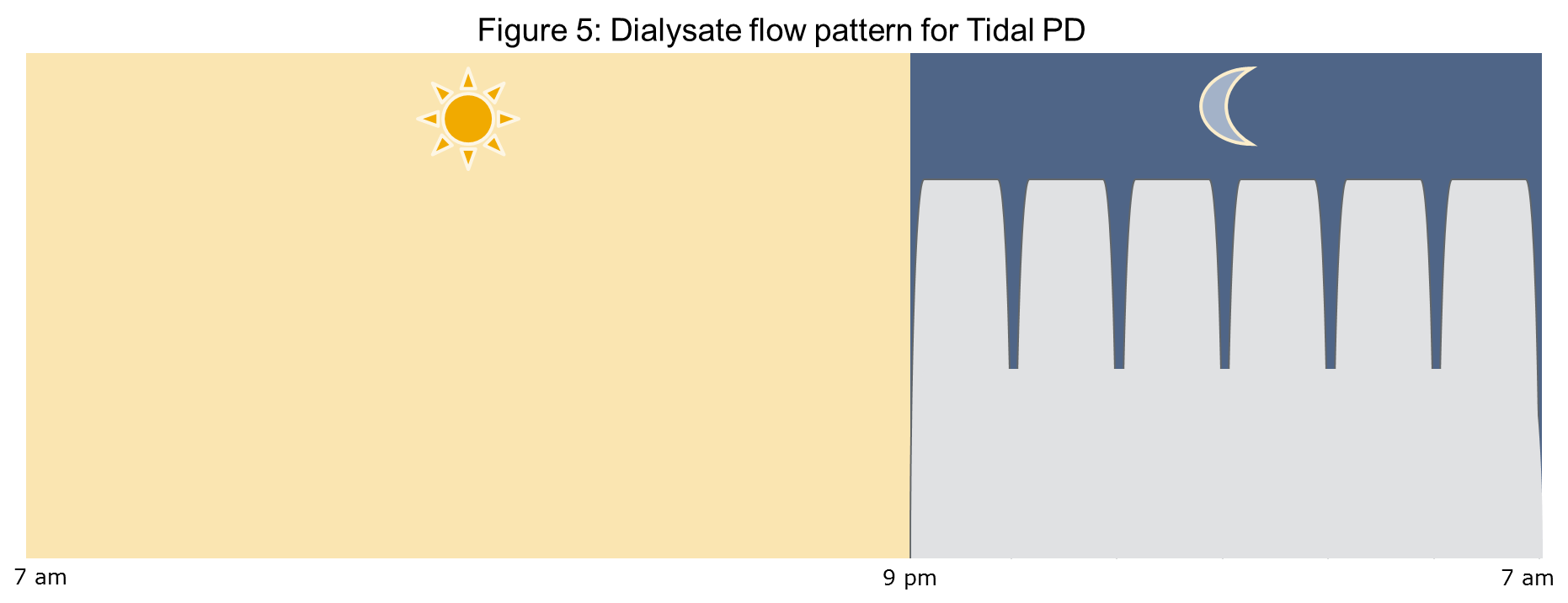
Tidal peritoneal dialysis (TPD) consists of an initial infusion of dialysate followed by a variable dwell and partial drain of the solution, leaving a residual volume in the peritoneal cavity until the final drain5. A tide is created during the partial infusions and drains that are performed. The initial fill is usually in the range of 2.0 to 2.5 L. The cavity is then partially drained where approximately 50% of the dialysate is drained, leaving a reserve volume. The cavity is then refilled. This is repeated until the end of the session when the cavity is completely drained. The cavity may be refilled for the daytime exchange. The principal purpose of TPD was to enhance clearance of small solutes by reducing the normal loss of dialytic time that is associated with the inflow and drainage of solution of the intermittent technique. Unfortunately, clinical experiences with TPD have not confirmed any advantage over APD in terms of clearance or ultrafiltration. Tidal PD may be useful for patients with inflow outflow pain, as well as those with slow drainage or multiple alarms due to drainage problems. The main disadvantages of TPD are its increased cost and complexity. The typical regimen is shown in figure 5.
Continuous flow peritoneal dialysis (CFPD)
CFPD is a modality of PD that uses the continuous technique and two separate catheters or a double lumen catheter15,16. This technique is performed with high dialysate flow rates and can help to reduce nondialytic time and maintain a constant intra-abdominal volume. PD fluid is infused into the peritoneal cavity through an inflow catheter while the outflow catheter is clamped. Once the desired fill volume is achieved, the outflow catheter is opened and the inflow and outflow are maintained relatively constant at high flow rates (150 – 250 mL/min)5. CFPD requires very large volumes of PD solution. Since it is impractical and economically prohibitive to use dialysis bags, several methods have been employed to solve this problem. Spent dialysate can be regenerated with hemodialysis technology. In other words, spent peritoneal dialysis solution is being “hemodialyzed”, instead of plasma water. Peritoneal dialysate can also be regenerated using sorbent technology. On-line generation of fluid is possible using hemodiafiltration technology or by mixing a concentrate with pure water. Potential advantages of CFPD include very high clearances, possible reduction in peritonitis and sustained ultrafiltration. While there has been much interest in CFPD for many years, the requirements of special peritoneal access and large volumes of solution have impeded its clinical application7.
References:
- Heimbürger O, Blake PG. Apparatus for Peritoneal Dialysis. In: Daugirdas JT, Blake PG, Ing TS, eds. Handbook of Dialysis. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2007:339-355.
- Popovich RPP, Moncrief JWW, Nolph KDD, Ghods AJJ, Twardowski ZJJ, Pyle WKK. Continuous ambulatory peritoneal dialysis. 1978. J Am Soc Nephrol. 1999;10(4):901-10. www.ncbi.nlm.nih.gov/pubmed/10203376
- Moncrief JW, Popovich RP, Nolph KD. The history and current status of continuous ambulatory peritoneal dialysis. Am J Kidney Dis. 1990;16(6):579-84. www.ncbi.nlm.nih.gov/pubmed/2239958
- Oreopoulos DG, Robson M, Izatt S, Clayton S, deVeber GA. A simple and safe technique for continuous ambulatory peritoneal dialysis (CAPD). Trans Am Soc Artif Intern Organs. 1978;24:484-9. www.ncbi.nlm.nih.gov/pubmed/716044
- Diaz-Buxo JA. Clinical Use of Peritoneal Dialysis. In: Nissenson AR, Fine RN, eds. Clinical Dialysis. 4th ed. New York: McGraw-Hill Medical Publication; 2005:421-490.
- Mujais S, Childers RW. Profiles of automated peritoneal dialysis prescriptions in the US 1997-2003. Kidney Int Suppl. 2006;(103):S84-90. www.ncbi.nlm.nih.gov/pubmed/17080117
- Khanna R, Krediet RT, eds. Nolph and Gokal’s Textbook of Peritoneal Dialysis. 3rd ed. New York: Springer Science+Business Media; 2009.
- Diaz-Buxo JA, Farmer CD, Walker PJ, Chandler JT, Holt KL. Continuous cyclic peritoneal dialysis: a preliminary report. Artif Organs. 1981;5(2):157-61. www.ncbi.nlm.nih.gov/pubmed/7271529
- Warady BA, Campoy SF, Gross SP, Sedman AB. Peritonitis with continuous ambulatory peritoneal dialysis and continuous cycling peritoneal dialysis. J Pediatr. 1984;105(5):726-30.
- Howard RL, Millspaugh J TI. Adults and pediatric peritonitis in a home dialysis program (Comparison of continuous ambulatory and continuous cycling peritoneal dialysis). Am J Kid Dis. 1990;16:469-472.
- Troidle LK, Gorban-Brennan N, Kliger AS FF. Continuous cycler therapy, manual peritoneal dialysis therapy, and peritonitis. Adv Perit Dial. 1998;14:137-141.
- Viglino G, Gandolfo C, Vigra G CP. Role of automated peritoneal dialysis within a peritoneal dialysis program. Adv Perit Dial. 1995;11:134-138.
- Gahl GM, Jörres A. Nightly intermittent peritoneal dialysis: targets and prescriptions. Perit Dial Int. 2000;20 Suppl 2:S89-92. www.ncbi.nlm.nih.gov/pubmed/10911650
- Woodrow G, Turney JH, Cook JA, Gibson J, Fletcher S, Stewart AJ, Brownjohn AM. Nocturnal intermittent peritoneal dialysis. Nephrol Dial Transplant. 1994;9(4):399-403. www.ncbi.nlm.nih.gov/pubmed/8084454
- Shinaberger JH, Shear L, Barry KG. Peritoneal-extracorporeal recirculation dialysis; a technique for improving efficiency of peritoneal dialysis. Invest Urol. 1965;2:555-66. www.ncbi.nlm.nih.gov/pubmed/14283599
- Diaz-Buxo JA. Evolution of continuous flow peritoneal dialysis and the current state of the art. Semin Dial. 2001;14(5):373-7. www.ncbi.nlm.nih.gov/pubmed/11679107
P/N 102483-01 Rev. A 12/2014